Intubation: Methods at a glance

Intubation is a procedure that is mainly used in anesthesia, intensive care and emergency medicine. It is used to secure the airways of unconscious, anaesthetized or sedated patients by inserting an endotracheal tube through which artificial respiration can be administered. There are different methods of intubation depending on the patient’s condition, anatomical circumstances and availability of aids. While classic direct laryngoscopy is still widely used, modern procedures such as video laryngoscopy or fiberoptic intubation are becoming increasingly important. There are also alternative access routes such as nasal intubation or coniotomy, which are particularly relevant in emergency situations.
In this article, we would like to give you an overview of the various techniques and how they are carried out.
Direct Laryngoscopy
Direct laryngoscopy is the classic method of intubation using a laryngoscope with a direct view of the vocal cords. The patient is placed in the “sniffing position” with the head slightly bent backwards and the neck extended. A laryngoscope with a Macintosh or Miller blade is then inserted into the mouth to displace the tongue to the side and make the glottis visible. An endotracheal tube is inserted through the vocal cords into the trachea and the correct position is checked.

Products used:
- Laryngoscopes,
- MIL or MAC blades
- Standard endotracheal tubes
Advantages:
- Proven and widely used method
- No expensive special equipment required
- Fast implementation for experienced users
Practical procedure:
The patient is placed in the “sniffing position”, with the head slightly bent backwards and the neck extended. A laryngoscope with a Macintosh or Miller blade is then inserted into the mouth to displace the tongue to the side and make the glottis visible. An endotracheal tube is inserted through the vocal cords into the trachea and the correct position is checked, for example by capnography or auscultation.
Videolaryngoscopy
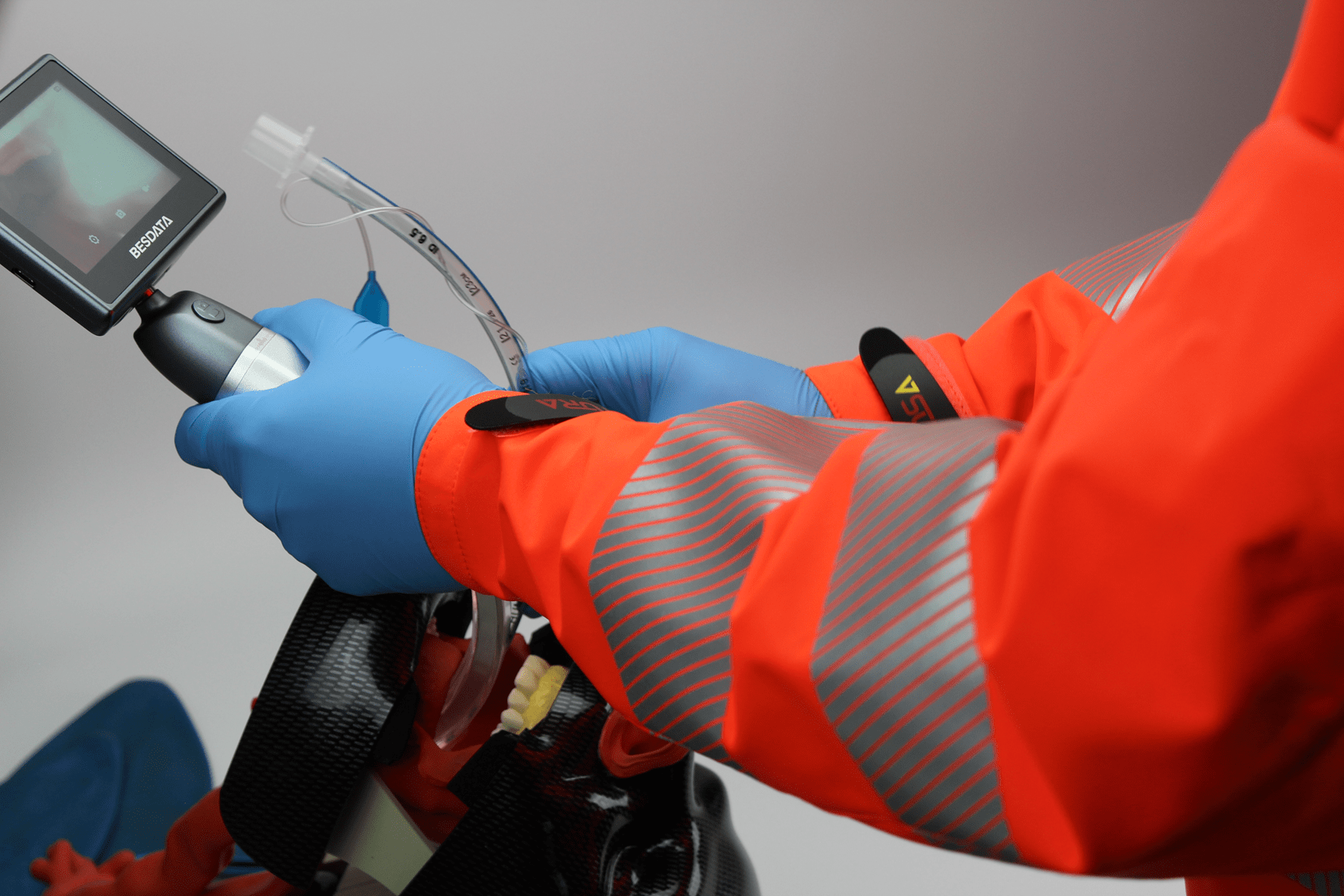
In video laryngoscopy, a laryngoscope with an integrated camera is used to display the vocal cords indirectly on a screen. The video laryngoscope is inserted without the need for a direct view of the vocal cords. The tube is placed under camera guidance and the correct position can be easily checked.
Relevance according to S1 Guideline Airway Management 2023: According to the current S1 guideline on airway management 2023 the use of video laryngoscopes is particularly recommended for difficult airways. The guideline emphasizes that video laryngoscopy has a higher initial intubation success rate compared to direct laryngoscopy and helps to reduce complications such as esophageal malpositions or tooth damage. Especially in emergency medicine and for less experienced users, video laryngoscopy is recommended as the preferred method to ensure safe intubation.

Products used:
- Videolaryngoscope (e.g.
VisionHEART video laryngoscope) - Disposable laryngoscope blade
- Possibly command staff
- Endotracheal tube
Advantages:
- Improved view of the glottis, especially with difficult airways
- Higher success rate than with direct laryngoscopy
- Particularly advantageous for less experienced users
Practical procedure:
The video laryngoscope is inserted centrally, with the patient’s gaze remaining fully focused on the screen. The glottis is identified under camera view, then the preformed endotracheal tube (field hockey position) is carefully advanced through the glottis. After cuff blocking, the position is checked using capnography, thoracic excursion and auscultation. Finally, the tube is fixed in place and ventilation is continued. This method offers better visibility and greater intubation safety, particularly in difficult airways.

Fiber optic Intubation
Fiberoptic intubation is performed using a flexible bronchoscope that allows direct visual control during intubation. The bronchoscope is inserted either orally or nasally to identify the vocal cords and push the tube into the trachea. This method is particularly suitable for awake intubations and difficult airways, but is more time-consuming and requires a lot of experience.
Products used:
- Flexible bronchoscopes
- Endotracheal tubes with large lumen
- Nasopharyngeal tube
Advantages:
- Ideal for awake intubation
- Particularly suitable for difficult airways
Practical procedure:
The bronchoscope is inserted orally or nasally until the glottis is visible. The endotracheal tube or nasopharyngeal tube is advanced into the trachea via the bronchoscope. Intubation can be performed with the patient awake or sedated, often with the support of local anesthetics to reduce the gag reflex.
Intubation via supraglottic airways
This method involves using aids such as laryngeal masks or laryngeal tubes, which are placed over the glottis and allow ventilation without the tube being inserted directly into the trachea. This method is a valuable alternative, particularly in emergency situations, if conventional intubation is not successful at the first attempt or the airway needs to be secured quickly.
Particular relevance in emergency medicine: Supraglottic intubation is a life-saving alternative in pre-hospital emergency situations or in difficult airways. It is particularly recommended if conventional endotracheal intubation is not immediately successful or is difficult for anatomical or traumatic reasons. Its ease of use allows even less experienced personnel to quickly secure the airway, making it an essential option in emergency management.

Products used:
- Laryngeal masks
- i-gel supraglottic airway aid
- Laryngeal tubes for emergency medicine
Advantages:
- Quick and easy to implement
- Particularly suitable for emergencies with a difficult airway
- No direct manipulation of the vocal cords required
- Rapid oxygenation in critical situations
Practical procedure:
After induction of anesthesia or deep sedation, the laryngeal mask or laryngeal tube is inserted into the mouth and advanced until it is correctly positioned over the glottis. The correct position is checked by capnography and observation of the thoracic excursion. In an emergency, a supraglottic airway device can be inserted within a few seconds to allow immediate oxygenation and ventilation. If definitive airway protection is required, subsequent endotracheal intubation via the laryngeal mask airway can be performed under certain conditions (so-called “second-step technique”).

Emergency - Coniotomy
Emergency coniotomy is the last resort when no other method of securing the airway is possible. It is used in a “can’t intubate, can’t oxygenate” (CICO) scenario. Access to the trachea is created via the anterior neck region by making a skin incision in the area of the cricothyroid ligament and inserting a tube or a coniotomy set.
Products used:
- Coniotomy sets
- Scalpel bougie technique
Advantages:
- Lifesaving in emergency situations
- Last option if no other method is possible
Practical procedure
The patient is placed in the supine position and the cricothyroid ligament is identified. A skin incision is made and an access to the trachea is created using a bougie or a special coniotomy set. A tube is then placed over the opening and secured.
Nasotracheal Intubation
Nasotracheal intubation is performed through the nose, with the tube being placed in the trachea under direct or fiberoptic visual control. After local anesthesia and vasoconstriction of the nasal mucosa, the tube is advanced through the nostril and finally placed in the correct position using a laryngoscope or bronchoscope.

Products used:
- Nasopharyngeal tube
- Magill pliers
- Nasal speculum
- Suction hose
- Goose gurgling for tube extension
Advantages:
- Ideal for awake intubation
- Particularly suitable for difficult airways
Practical procedure:
After local anesthesia and vasoconstriction of the nasal mucosa, the tube is carefully inserted through the nostril and advanced along the nasal floor. As soon as the tube reaches the pharynx, it is advanced with the aid of a laryngoscope or bronchoscope and Magil forceps and placed in the trachea.
What is the best method?
The choice of the correct intubation method depends on the situation, the patient’s condition and the experience of the practitioner. While modern techniques such as video laryngoscopy and fiberoptic intubation improve safety and success rates, direct laryngoscopy remains a proven standard method. In emergencies where no other option is available, coniotomy may be necessary as a last resort.